위암
이론과 하이라이트 히스토리를 확인 할 수 있어요.
위암
1. 위선암 (Gastric adenocarcinoma)
• 위에서 발생하는 암의 90%는 선암
1) 병리학적 분류
위 선암은 두가지 주요 형태로 나뉜다:
① Intestinal type (장형)
• 궤양을 동반하는 bulky, exophytic mass를 주로 형성
• 샘 구조로 증식함; 암세포는 다량의 apical mucin vacuole을 지니며 종양 중심 또는 생감에 다량의 점액이 축적됨
② Diffuse type (미만형)
• 개별 세포 또는 소집단 형태로 위벽을 광범위하게 침윤; 샘 구조를 형성하지 않음
- 접착력 상실(E-cadherin 소실)로 인해 세포가 유착력을 잃고 discohesive한 형태로 넓게 퍼짐
• 암세포는 큰 점액 공포가 세포질을 밀어내며 signet-ring cell 모양을 이룸
• 침윤 부위에서 섬유반응(desmoplasia)을 유발하여 위벽이 단단해지고 두꺼워짐 → 병변이 광점위할 경우 rugae와 같음 점막의 주름을 소실하고 가죽과 같은 위벽을 형성하며 이를 linitis plastica라고 칭함
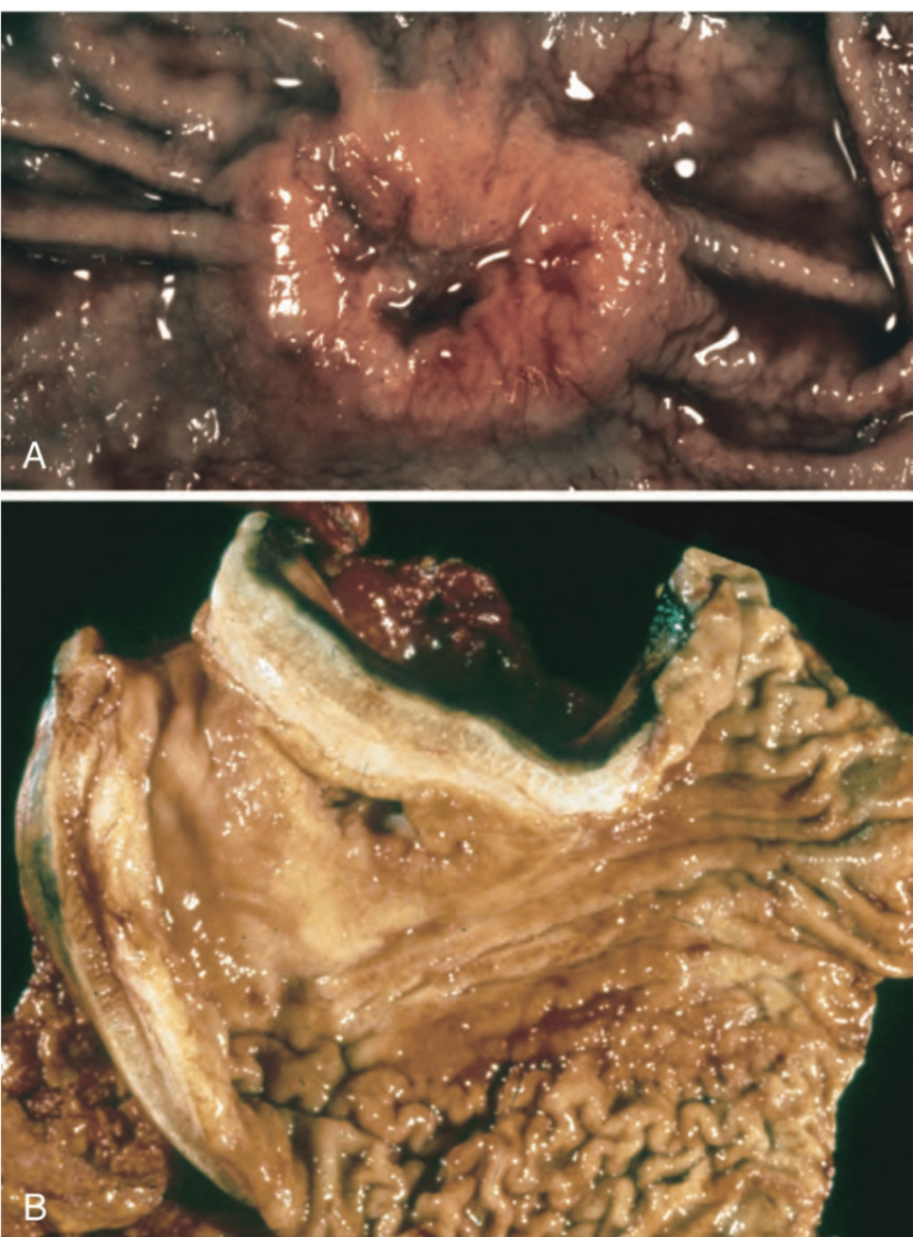
B: infiltrative type (linitis plastica) gastric cancer
Robbins and Cotran Pathologic Basis of Disease, 10e, pg 775
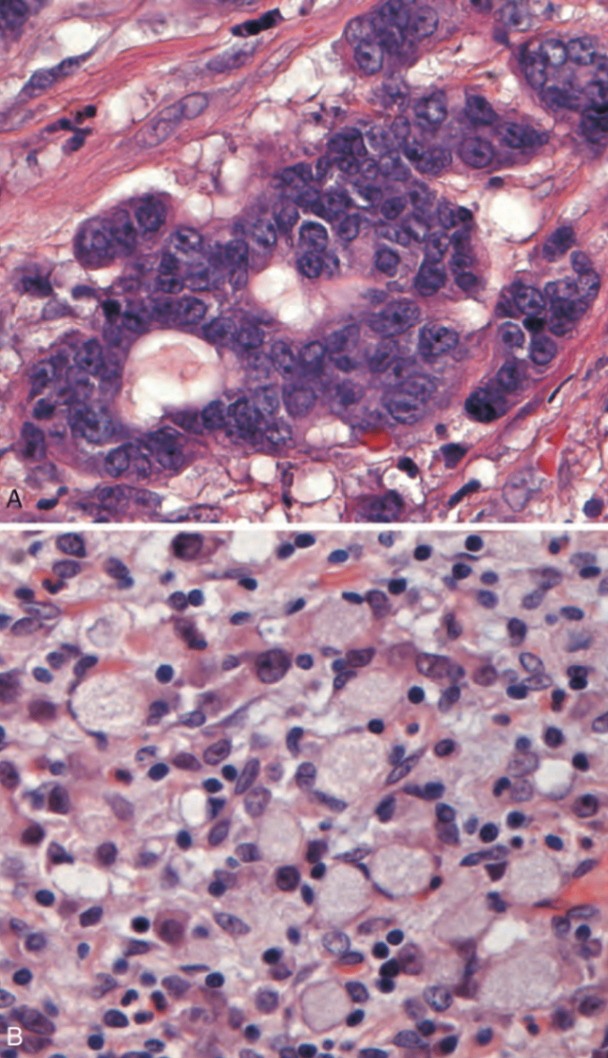
A: intestinal-type adenocarcinoma
B: infiltrative type gastric cancer
Robbins and Cotran Pathologic Basis of Disease, 10e, pg 776
2) 분자 병인
① Intestinal type (장형)
• Wnt 신호 경로 활성화가 주된 분자 병인
- APC 종양억제유전자 소실
※ familial adenomatous polyposis (FAP, germline APC mutation) intestinal-type 위암 위험 증가
- β-catenin gain-of-function mutation
→ 결과적으로 세포 증식 및 생존 신호 증가
② Diffuse type (미만형)
• E-cadherin(CDH1) 유전자 기능 소실
- 세포 간 접착력 상실
- 세포 분극 및 구조 유지 기능 저하
→ 세포의 확산성과 침윤성을 증가시킴
3) 임상적 함의
• 장형은 H.pylori 감염, 위축성 위염 등과 같은 환경 요인과 연관
• 미만형은 유전적 요인의 영향이 강함
• 예후는 병기 및 병리형에 따라 다르며, 미만형이 일반적으로 더 예후 불량
4) 병기
• 위암의 병기 TNM 중 tumor, 즉 원발 종양 깊이가 가장 중요한 예후 인지임
• 위암 병기의 T stage (primary tumor의 depth of invasion)는 다음과 같이 분류된다:
T0 | No evidence of primary tumor |
Tis | Carcinoma-in-situ; intraepithelial tumor without invasion of lamina propria |
T1 | Tumor invades the lamina propria, the muscularis mucosa or the submucosa |
T1a | Tumor invades the lamina propria or muscularis mucosa |
T1b | Tumor invades the submucosa |
T2 | Tumor invades the muscularis propria layer |
T3 | Tumor invades the subserosa layer without invasion of the serosa and adjacent structures |
T4 | Tumor penetrates the serosa (visceral peritoneum) or adjacent structures |
T4a | Tumor penetrates the serosa (visceral peritoneum) |
T4b | Tumor invades adjacent structures |
2. Extranodal marginal zone B-cell lymphoma of MALT type
1) 개요
• MALToma는 extranodal marginal zone B-cell lymphoma의 일종으로, mucosa associated lymphoid tissue9(MALT)에서 유래하는 저등급 (non-Hodgkin) B세포 림프종
• Extranodal lymphoma는 어디서든 생길 수 있지만, 가장 흔한 부위는 소화기계, 특히 위이다
2) 병태생리
• 정상 위점막에서는 MALT가 없음
• 그러나 만성 위염, 특히 H.pylori 감염에 의해 MALT가 유도됨
• 이처럼 이소성 MALT가 형성된 부위에서 림프종이 발생
→ H.pylori는 위 MALToma의 가장 흔한 유발 요인
3) 병리학적 특징
• Lamina propria에 밀집된 B 림프구 침윤
• Lymphoepithelial lesion 형성: 종양성 림프구가 위샘을 침윤하여 샘 구조를 파괴
• B cell secondary follicle가 종종 함께 존재
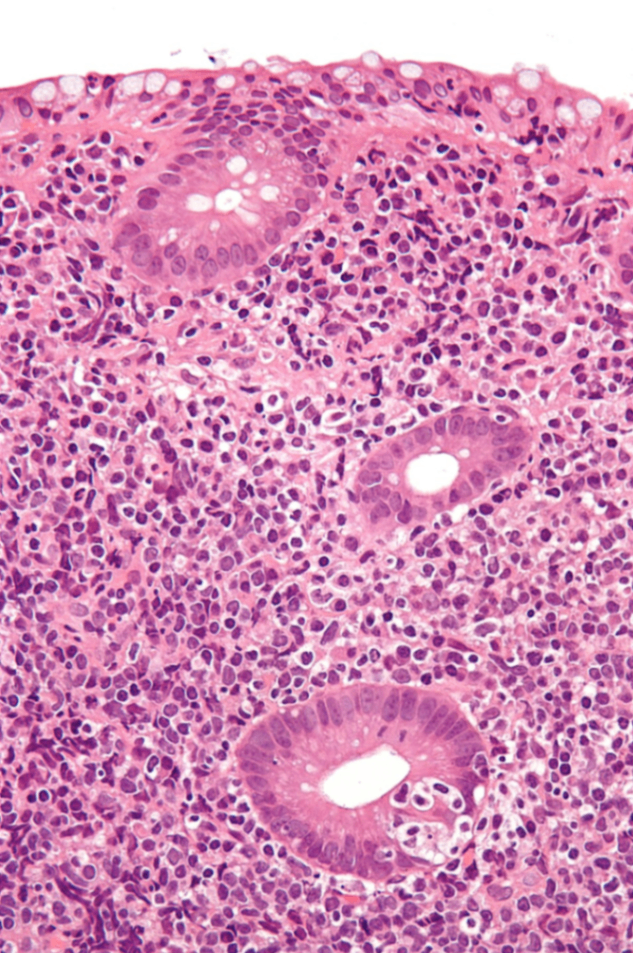
• 면역표현형: 성숙 B세포 기원이므로 CD19+, CD20+ (CD5, CD10는 보통 음성)
4) 임상적 특징
• 조기 병기에서는 비교적 느린 성장 속도와 양호한 예후
• 많은 경우 H.pylori 제균 치료만으로도 완전 관해 가능
3. Gastrointestinal stromal tumor, GIST
• 위장관에서 발생하는 가장 흔한 mesenchymal 종양
1) 기원 및 분자병리
• 기원세포: interstitial cells of Cajal, 장의 자율 운동 조절을 담당하는 기질 내 pacemaker 세포
• 주요 유전자 이상:
- 약 75%는 receptor tyrosine kinase인 KIT (CD117)의 gain-of-function mutation 보유
- 일부는 KIT의 하위 경로의 signaling receptor인 PDGFRA 활성화 돌연변이 보유
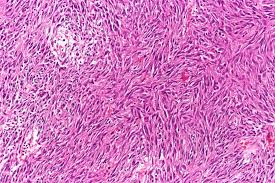
2) 조직학적 소견
• 단일, 주변 조직과의 경계가 뚜렷한 종괴
• 대개 점막하층 또는 근육층에서 발생
• 세포 형태:
- spindle cell type: 가장 흔함
- epitheliod type도 존재
- 핵 다형성은 일반적으로 드묾
3) 면역조직화학
• KIT (CD117)가 가장 중요한 진단 마커: 90-95% 양성
Reference: Robbins and Cotran, Pathologic Basis of Disease, 10e