호흡기계 발달
이론과 하이라이트 히스토리를 확인 할 수 있어요.
1. 개요
1) 호흡기계는 conducting portion과 respiratory portion으로 나뉜다.
① Conducting portion: 공기를 전달, 가습 및 온도 조절 (nasal cavity → terminal bronchioles)
② Respiratory portion: 실제 가스 교환이 일어나는 부위 (respiratory bronchioles, alveoli)
2) 발생학적으로는 upper respiratory tract와 lower respiratory tract로 나뉜다.
① Upper respiratory tract: nasal cavity, oral cavity, pharynx
② Lower respiratory tract: trachea, bronchi, bronchioles, alveoli
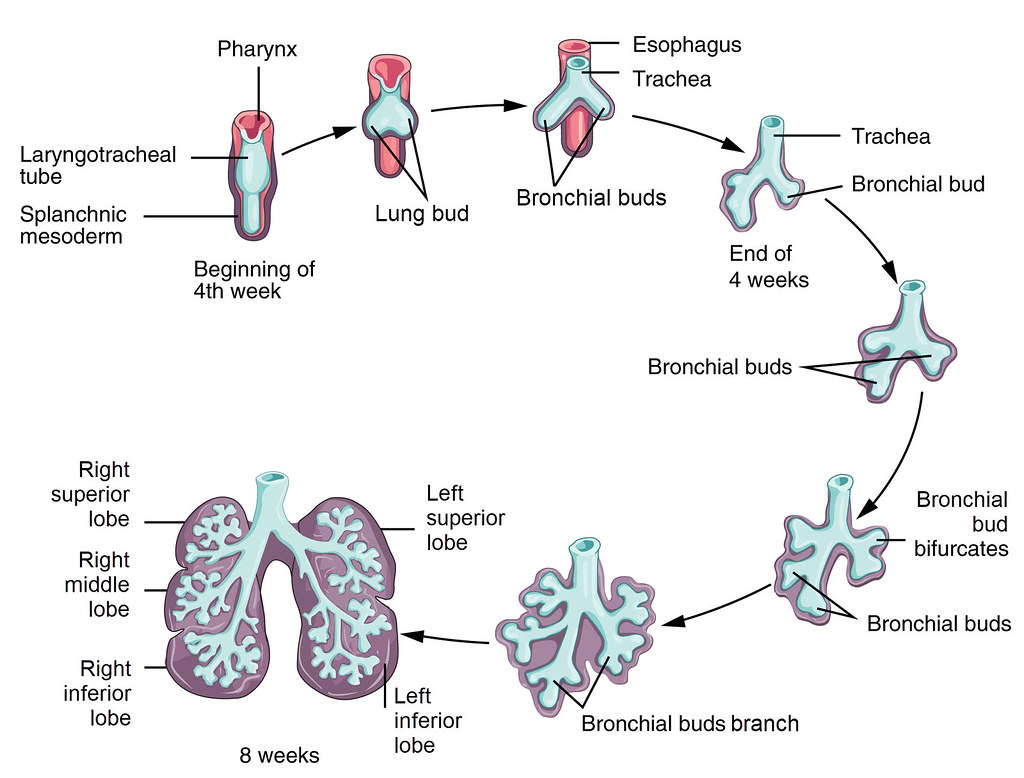
2. 초기 발생 (4주차)
: 호흡기계는 foregut (primitive gut tube의 anterior portion)에서 기원한다.
1) respiratory diverticulum이 foregut에서 ventral 쪽으로 돌출됨
2) 이후 tracheoesophageal septum이 형성되어 식도와 기관 분리됨
3) diverticulum이 primary bronchi로 나뉘며, 계속 분지하여 bronchial tree를 형성함
3. 호흡기계 발생 단계
단계 | 주차 | 주요 특징 |
|---|---|---|
Pseudoglandular | Week 8–16 | Bronchioles 형성, alveoli는 없음 → gas exchange 불가 |
Canalicular | Week 16–26 | respiratory bronchioles 형성 시작, 혈관 침투, 생존율 낮음 |
Terminal sac | Week 26~ | Type I pneumocyte (가스교환), Type II pneumocyte (surfactant 생성) 형성 시작 |
Alveolar | Late fetal → postnatal | alveoli 수 증가 및 성숙, 출생 후 몇 년까지 지속 |
4. 횡격막의 발달
: 횡격막(diaphragm)은 다음 4가지 구조가 융합되어 형성된다:
구성 요소 | 발생 시기 | 기원 |
|---|---|---|
Septum transversum | Week 4 | 앞쪽 횡격막 형성 (간과 심장 사이의 중격 역할) |
Pleuroperitoneal membranes | Week 5–6 | 후외측부 막 형성 → 복강과 흉강 분리 |
Dorsal mesentery of esophagus | Week 6 | 중앙 부분 → crura 형성 |
Body wall mesenchyme | Late fetal period | 말초부 → 근육 확장 |
5. 임상적 연관 포인트
1) Tracheoesophageal Fistula
(1) trachea와 esophagus가 완전히 분리되지 못하면 누공 형성
(2) 증상: feeding 시 cyanosis, aspiration, regurgitation
(3) 치료: 수술적 교정 필요
2) Respiratory Distress Syndrome (RDS)
(1) Type II pneumocyte 미성숙 → surfactant 부족
(2) alveoli 확장 어려움 → 첫 호흡 실패, 청색증
(3) 치료 및 예방:
① 출산 전 glucocorticoid 투여 → surfactant 생성 유도
② 출생 후 인공 surfactant 투여 및 산소 요법